Liver Cirrhosis
At CLRD, we care for people living with cirrhosis by combining advanced regenerative therapies with personalized medical care. Cirrhosis can feel overwhelming, fatigue, swelling, and frequent hospital visits can disrupt daily life, but you are not alone. Our patient-centric programs focus on restoring liver function, easing symptoms, and improving quality of life. Using autologous bone marrow stem cells delivered via the hepatic artery, along with comprehensive cirrhosis care, our teams have helped patients stabilize and recover, often reducing the need for liver transplantation and enabling a return to everyday routines. Every treatment is tailored to your stage of disease, your goals, and your support system, so progress is measured not only in lab values but in stronger days with fewer complications and more confidence in the future.
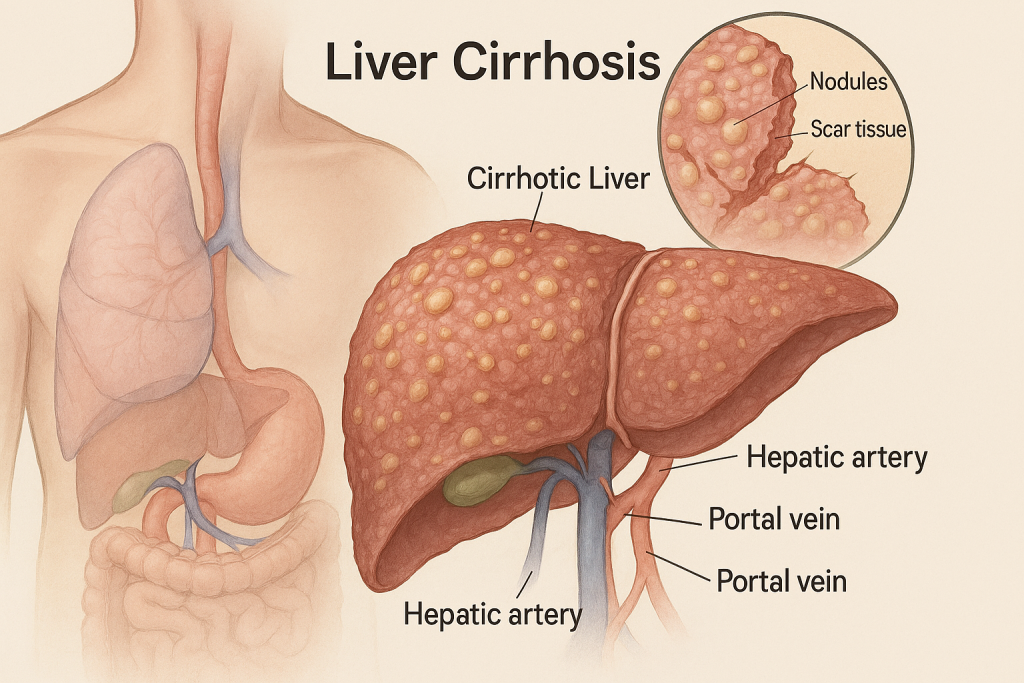
Cirrhosis develops when chronic injury triggers scarring that distorts normal liver architecture and impairs function. At CLRD, our flagship intervention, autologous bone marrow stem cell transplantation via the hepatic artery, is designed to biologically support and regenerate injured parenchyma. In carefully selected patients with compensated or early decompensated cirrhosis, we perform angiographic infusion of a defined dose of their own mesenchymal stem cells into the proper hepatic artery, targeting widespread intrahepatic delivery. This approach has shown clinically meaningful improvements in bilirubin, albumin, and prothrombin activity, with reductions in Model for End-Stage Liver Disease (MELD) and Child–Pugh scores and better short- to mid‑term survival, aligning with published controlled trials and meta‑analyses that favor arterial infusion over venous routes for enhanced efficacy. In our program, patients typically experience measurable gains by 2–4 weeks, with benefits sustained for months; repeat dosing and supportive medical therapy are individualized based on response, etiology, and portal hemodynamics. For those presenting with acute‑on‑chronic liver failure (ACLF), our cirrhosis pathways integrate intensive supportive care and stem‑cell–based rescue where appropriate, reflecting evidence that the ACLF subgroup may derive particular functional benefit from MSC therapy without increased adverse events. Across these pathways, our capability extends beyond procedure delivery: rigorous pre‑infusion optimization (nutrition, micronutrients, infection control), portal‑pressure–aware management of ascites and varices, and structured follow‑up (encephalopathy prevention, vaccination, bone health, and lifestyle support) help translate biological gains into day‑to‑day improvements and fewer hospitalizations. For patients not eligible for immediate transplantation, or those seeking to delay it, our regenerative protocols offer a practical bridge that can restore performance status and expand future options.
Symptoms
People often notice tiredness, poor appetite, easy bruising, itching, abdominal swelling (ascites), leg edema, yellowing of the eyes/skin (jaundice), and sometimes confusion or sleepiness from hepatic encephalopathy. Some may develop muscle loss, dark urine, pale stools, or upper‑abdominal discomfort. As symptoms intensify, they can interfere with work, sleep, and social activity, but many improve as liver function recovers after our targeted therapy and comprehensive care.
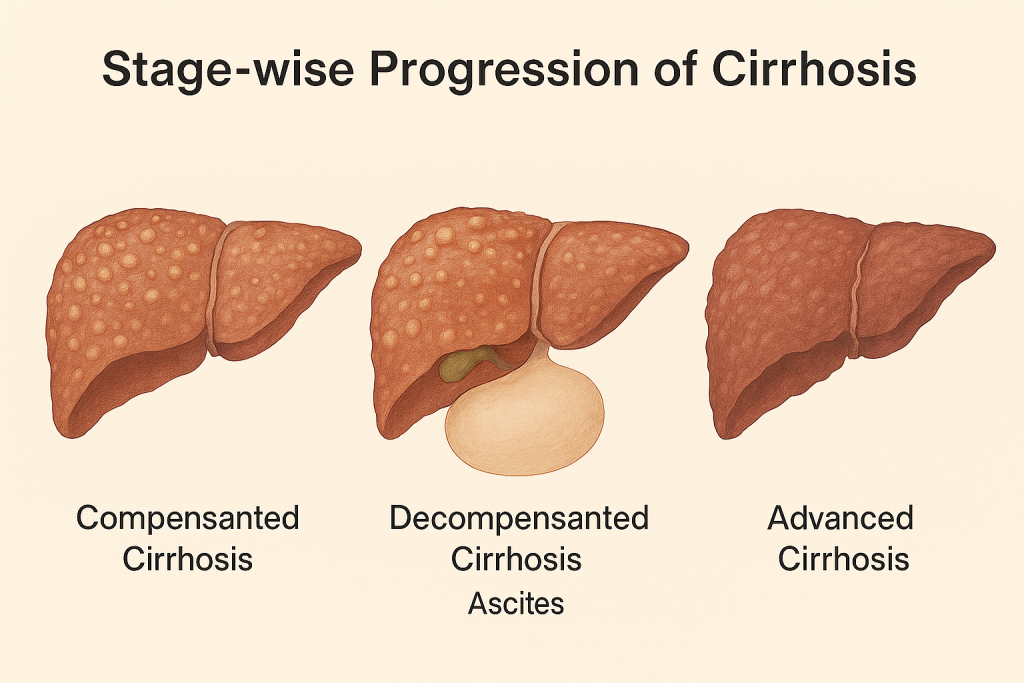
Stage-wise Progression
- Compensated Cirrhosis: Scarring is present but the liver still manages its tasks. People may feel well with occasional fatigue or mild lab abnormalities. We focus on surveillance and early intervention, autologous stem‑cell infusion is considered here to prevent decompensation, taking advantage of evidence for early functional gains.
- Decompensated Cirrhosis: Fluid accumulation in the abdomen, variceal bleeding risk, and encephalopathy emerge. Our protocols combine MSC therapy (arterial infusion where appropriate), diuretics, paracentesis planning, variceal prophylaxis, nutrition, and infection control to restore stability and reduce readmissions, mirroring data that show improved albumin, bilirubin, and survival after MSC therapy, especially in higher‑risk subsets like ACLF.
- Advanced/Transplant‑Threshold Cirrhosis: Multi‑system complications and low synthetic function can necessitate transplant evaluation. For patients not immediately eligible or seeking delay, our regenerative pathway offers a bridge, targeting MELD and Child–Pugh improvements and functional recovery that may expand future options and support candidacy while improving daily quality of life.
Our Treatment Capabilities
Many people come to us at different points in their cirrhosis journey. One common scenario is viral‑related cirrhosis (past HBV/HCV) where fatigue, ankle swelling, and mild jaundice gradually appear; with timely stem‑cell infusion and optimized antiviral care, patients often see bilirubin fall and albumin rise, translating into more energy and fewer clinic visits. Another frequent scenario is metabolic/NAFLD‑related cirrhosis in individuals managing diabetes and weight concerns; here, controlled MSC therapy paired with nutrition and exercise support can lessen ascites, improve coagulation parameters, and help patients resume routine activities. We also care for alcohol‑associated cirrhosis after sustained abstinence, where stem‑cell infusion complements counseling and relapse‑prevention, resulting in noticeable improvements in MELD and Child–Pugh scores and a reduced need for large‑volume paracentesis. In those with autoimmune or cholestatic cirrhosis, our protocols coordinate immunomodulatory medicines with regenerative therapy to stabilize cholestasis and reduce pruritus, while closely monitoring portal pressures and variceal risk. For patients presenting with ACLF, sudden worsening on a background of cirrhosis with jaundice, coagulopathy, and confusion, we deliver rapid supportive care and, where suitable, targeted MSC rescue to help reverse metabolic instability and shorten intensive care stays, consistent with published long‑term follow‑up showing improved survival and functional indices with multi‑dose MSC regimens. Throughout, our aim is straightforward: fewer complications, better function, and a life lived less around hospital schedules and more around what matters to you.